Laboratory Methods
This section includes an instructional video describing specimen collection techniques from skin, hair and nails for the laboratory diagnosis of tinea, ringworm and onychomycosis, together with information on methods for antifungal susceptibility testing and recipes for microscopy stains and culture media.
-
Antifungal susceptibility testing

Equipment needed for antifungal susceptibility testing.
Antifungal susceptibility testing (AFST) results are influenced by methodological factors, including: (i) isolate growth phase and inoculum size; (ii) incubation time and temperature; (iii) media type, particularly relating to glucose concentration; (iv) purity, concentration and activity of the antifungal agent; (v) endpoint stringency (e.g. 50%, 90%, or 100% growth inhibition); and (vi) whether these endpoints are read visually or spectrophotometrically. This wide range of variables formed the rationale for developing methodology standards by CLSI and EUCAST. Each method is time tested, accurate and reliable, but labour-intensive and requires significant training of staff, maintenance of expertise, and a large volume of isolates to be cost effective. Due to methodological differences, CLSI and EUCAST standard methodologies often yield different MICs and must therefore only be interpreted using the applicable breakpoints.
CLSI M27-A4 standard for yeasts:
See CLSI. Reference Method for Broth Dilution Antifungal Susceptibility Testing of Yeasts; Approved Standard - Fourth Edition. CLSI document M27-A4. CLSI, Pennsylvania, USA 2017.The M27-A4 standard is intended for testing yeasts including Candida species and Cryptococcus species (C. neoformans and C. gattii) by using either a macro or micro broth dilution test system. It recommends the use of RPMI-1640 medium with glutamine and phenol red without bicarbonate, inoculum standardized to 0.5 McFarland using a densitometer, and incubation at 35oC. Endpoints are read at 24 hours for non-fastidious yeasts like Candida or at 48 to 72 hours for slower growing yeasts like Cryptococcus.
The microdilution wells should be visualised with the aid of a reading mirror and the growth in each well should be compared with that of the growth control. A numerical score from 0 to 4 is given to each well using the following scale:
0 = optically clear
1 = slightly hazy
2 = prominent reduction in turbidity compared with that of the drug-free growth control
3 = slight reduction in turbidity compared with that of the drug-free growth control
4 = no reduction in turbidity compared with that of the drug-free growth controlThe MIC for amphotericin B is the lowest concentration with a score of 0 (optically clear, 100% growth inhibition). The MICs for the azoles, 5-fluorocytosine and the echinocandins are the lowest concentrations with a score of 2 (prominent decrease in turbidity, approx. 50% growth inhibition).
Interpretation of results:
The CLSI has endorsed Clinical Breakpoints (CBPs) for the echinocandins, voriconazole and fluconazole against several Candida species.3 Importantly, all previous CLSI interpretive criteria (e.g. itraconazole, 5-fluorocytosine) are now considered obsolete and must not be used.3 Breakpoints developed from any other methodology must not be used to interpret CLSI broth microdilution MICs. Additionally, in the absence of CBPs, epidemiological cutoff values (ECVs) have been developed and endorsed for many species, including Cryptococcus spp.4Clinical breakpoints (CBPs) and Epidemiological Cut-Off (ECV) values based on MICs or MECs for Candida and Aspergillus species as endorsed by CLSI.3,4 Note that some genotype-specific CLSI ECVs are now available for Cryptococcus species, but require molecular typing for valid use.4
EUCAST for yeasts: http://www.eucast.org/ast_of_fungi/
The European Committee on Antimicrobial Susceptibility Testing–Subcommittee on Antifungal Susceptibility Testing (EUCAST‐AFST) provides methodology for the testing of non‐fermentative yeasts, most importantly for Candida and Cryptococcus.
The current standard for yeasts is EUCAST definitive document EDef 7.3.1: Method for the determination of broth dilution minimum inhibitory concentrations of antifungal agents for yeasts.Note: Due to methodological differences, CLSI and EUCAST standard methodologies often yield different MICs and must therefore only be interpreted using the applicable breakpoints. ie you can not use EUCAST breakpoints for interpreting CLSI test procedures and vice versa.
EUCAST clinical breakpoints for Candida and Aspergillus (pdf).
EUCAST DEFINITIVE DOCUMENT E.DEF 7.3. (pdf)Essential differences between CLSI and EUCAST broth microdilution standard methodologies for yeasts.
Characteristics CLSI M27-A4 EUCAST Edef 7.3.1
Format Round based wells Flat based wells Final Inoculum 0.5 - 2.5 x 103 CFU/mL
0.5 - 2.5 x 105 CFU/mL
Test medium RPMI 1640 with 0.2% glucose RPMI 1640 with 2% glucose Growth Temperature 35°C 35°C Incubation time 24-48 h
Except: 72 h for Cryptococcus18-24 h
Except: 24-48 h for CryptococcusEndpoint 50% inhibition
Except: 90% inhibition AmB50% inhibition
Except: 90% inhibition AmBReading Visually Spectrophotometer CLSI M38-A3 standard for moulds:
See CLSI. Reference Method for Broth Dilution Antifungal Susceptibility Testing of Filamentous Fungi; Approved Standard. CLSI document M38-A3. CLSI, Pennsylvania, USA 2017.
The M38-A3 standard describes a method for testing antifungal susceptibility of filamentous fungi (moulds) that cause invasive infections, including Aspergillus spp., Fusarium spp., Scedosporium spp., zygomycetes and other pathogenic moulds. It recommends the use of RPMI-1640 medium (with glutamine, without bicarbonate, and with phenol red as a pH indicator.
However for the moulds the inoculum preparation of conidial or sporangiospores suspensions must be adjusted using a spectrophotometer with a test inoculum in the range 0.4x104 to 5x104 CFU/mlL providing the most reproducible MIC data. The optical density (OD) at 530nm required is dependant on the conidial or sporangiospores size of the mould being tested; i.e. for Aspergillus and Sporothrix species the OD = 0.09-0.11; for Fusarium, Scedosporium/Lomentospora, and Rhizopus species the OD = 0.15-0.17; for Bipolaris and Histoplasma species the OD = 0.2.Microdilution trays are incubated at 35oC; and may be read at 24 hours for Rhizopus species; 48 hours for Aspergillus, Fusarium and Sporothrix species; and 72 hours for slower growing moulds like Scedosporium/Lomentospora species. Most moulds may be read at 48 hours. Turbidity in the microdilution wells should be scored with the aid of a reading mirror and compared with that of the growth control. A numerical score from 0 to 4 is given to each well using the following scale:
0 = optically clear or absence of growth
1 = slight growth (25% of growth control)
2 = prominent reduction in growth (50% of growth control)
3 = slight reduction in growth (75% of growth control)
4 = no reduction in growthThe MIC for amphotericin B, itraconazole, voriconazole and posaconazole is the lowest concentration with a score of 0 (optically clear, 100% inhibition). The MICs for 5-fluorocytosine and fluconazole are the lowest concentrations with a score of 2 or lower (50% growth reduction). Echinocandin endpoints should be read as the minimum effective concentration (MEC) at which ‘aberrant growth’ occurs, that is, morphological change from filamentous hyphal growth to the granular ‘compact hyphal balls’ appearance.
Interpretation of results:
For Amphotericin B endpoints are typically well defined with most moulds clustering between 0.5 and 2.0 μg/ml. However some species such as Aspergillus terreus, Acremonium strictum, Scedosporium apiospermum and Scedosporium/Lomentospora (Scedosporium) prolificans show higher MICs in the range of 2 to 16 μg/ml (although very little data are available, MICs above 2 μg/ml have been associated with treatment failures). RPMI medium may also be unreliable in detecting resistance to Amphotericin B. For 5-fluorocytosine most mould MICs are greater than 64 μg/ml, the only exception are some isolates Aspergillus and the dematiaceous fungi. Similarly for fluconazole most mould MICs are greater than 64 μg/ml, the only exception are some isolates of the dimorphic fungi and dermatophytes. For itraconazole, voriconazole and posaconazole the endpoints are typically well defined with MICs ranging from 0.0313 to 16 μg/ml. No CLSI clinical breakpoints have been published for moulds MICs and there is very limited in vivo data available. However, ECVs have been endorsed for some Aspergillus species, which may be used on clinical reports.4Clinical breakpoints (CBPs) and Epidemiological Cut-Off (ECV) values based on MICs or MECs for Candida and Aspergillus species as endorsed by CLSI.3,4 Note that some genotype-specific CLSI ECVs are now available for Cryptococcus species, but require molecular typing for valid use.4
EUCAST for moulds: http://www.eucast.org/ast_of_fungi/
The European Committee on Antimicrobial Susceptibility Testing–Subcommittee on Antifungal Susceptibility Testing (EUCAST‐AFST) provides methodology for the testing of conidia forming moulds.
The current standard for yeasts is EUCAST definitive document EDef 9.3.1: Method for the determination of broth dilution minimum inhibitory concentrations of antifungal agents for conidia forming moulds.
Note: Due to methodological differences, CLSI and EUCAST standard methodologies often yield different MICs and must therefore only be interpreted using the applicable breakpoints. ie you can not use EUCAST breakpoints for interpreting CLSI test procedures and vice versa.
EUCAST clinical breakpoints for Candida and Aspergillus (pdf).
EUCAST DEFINITIVE DOCUMENT E.DEF 9.3.1(pdf).Essential differences between CLSI and EUCAST broth microdilution standard methodologies for moulds.
Characteristics CLSI M38-A3 EUCAST Edef 9.3.1 Format Round based wells Flat based wells Final Inoculum 0.4 - 5 x 104 CFU/mL
1 - 2.5 x 105 CFU/mL
Test medium RPMI 1640 with 0.2% glucose RPMI 1640 with 0.2% glucose Growth Temperature 35°C 35°C Incubation time 48 h (21-74 h) 48 h (24-72 h) Endpoint 100% inhibition
Except: aberrant growth (MEC) for echinocandins100% inhibition
Except: aberrant growth (MEC) for echinocandinsReading Visually Visually
Commercially available AFST systems:
Current workload pressures in laboratories, coupled with a structure of rotating non-specialised staff, do not align with routine use of reference AFST methods. Instead the use of commercial tests offers many practical advantages.5,6,7,8
Sensititre YeastOne Test Panel (Pichia kudriavzevii).
Sensititre® YeastOne™ Test Panel:
(Manufactured by TREK but supplied in Australia by Thermofisher Scientific). This ‘CLSI-compatible’ colorimetric broth microdilution method shares fundamental aspects of its procedure with the CLSI standard and has well established performance equivalence with the CLSI standard.8,10,11 Each test consists of a disposable microtitre plate, which contains dried serial dilutions of up to nine antifungal agents (YO10 panel), The wells also contain Alamar Blue as a colorimetric indicator, which assists endpoint reading with a colour change from blue to pink. Critically, this method must only be used in association with current CLSI-endorsed CBPs and ECVs. 5,6,7Sensititre® YeastOne™ Test Instructions (pdf)
Overall, the Sensititre YeastOne is a robust and reproducible test, easy to set up, the end points are clearly visible and it has a long shelf life. The test also works with moulds, especially those that sporulate freely like Aspergillus. Note that echinocandin-mould endpoints are ambiguous with this method, and the well colour should be ignored. Rather, the endpoint should be read in the same way as for the CLSI standard, that is the lowest concentration at which morphological change from filamentous hyphal growth to the granular ‘compact hyphal balls’ is observed.2
Endpoint reading of echinocandin antifungals (caspofungin, anidulafungin, micafungin) against Aspergillus spp. using Sensititre YeastOne.

Note: The minimum effective concentration (MEC) should be read as the lowest drug concentration causing aberrant growth - change in hyphal morphology from unbranched ‘fluffy’ growth (wells 1-2) to granular ‘compact hyphal balls’ (wells 3-11). Note that all wells become pink, and colour change should not be used to determine endpoint. Misreading the endpoint as an MIC (100% growth inhibition) will lead to reporting inaccurate results, and negatively impact treatment choices.
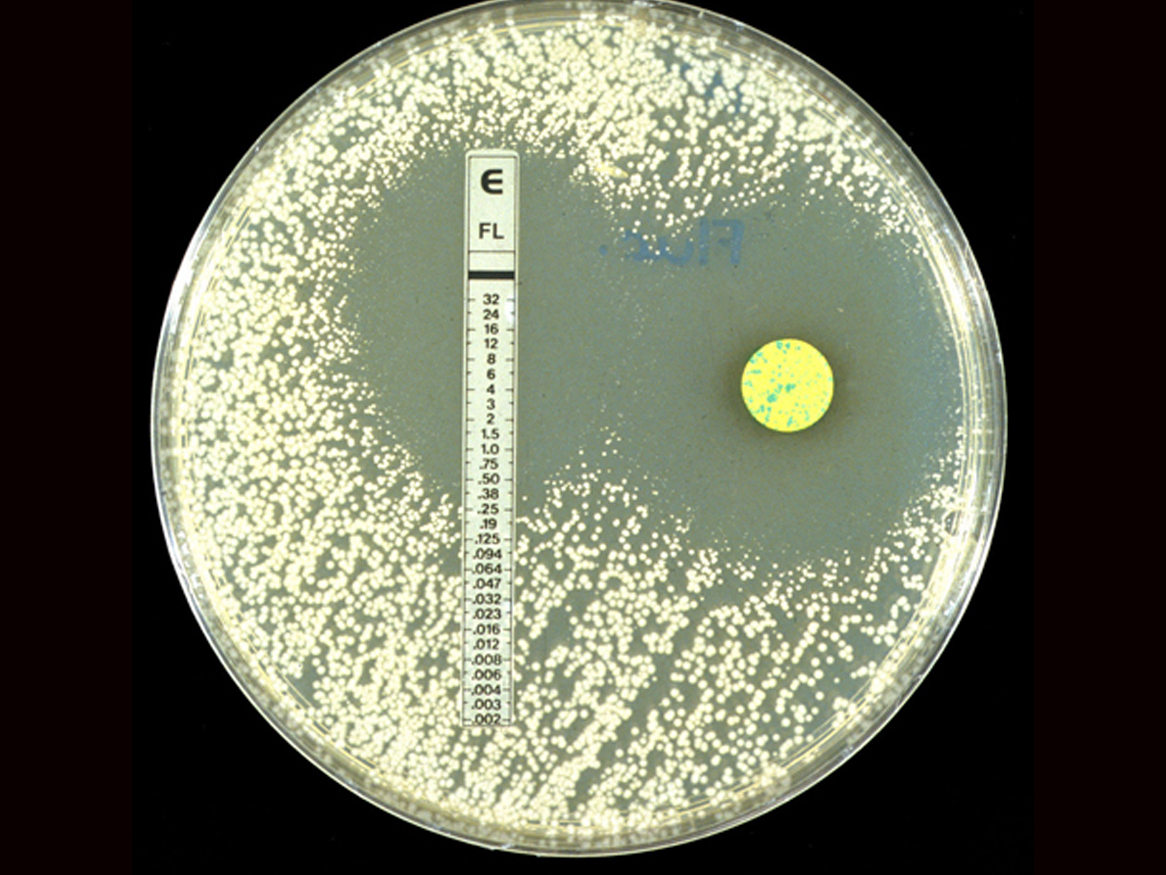
ETest®
(Manufactured by AB Biodisk in Sweden and supplied in Australia by Biomérieux). This is an agar diffusion method using a strip with a predefined concentration gradient of the antimicrobial agent being tested. This gradient allows for an MIC determination to be made. Etests have been extensively used for susceptibility testing of bacteria and they are also available for many antifungal agents. The two difficulties with Etests against fungi have always been which medium to use and with the interpretation of the endpoint. The latter problem remains but it is now recommended that modified RPMI-1640 agar supplemented with 0.2% glucose be used, in line with the CLSI standard.9,10,11Etests are simple to perform and the methodology is similar to that used in bacteriology. Individual antifungals may be tested and there is reasonable correlation with the CLSI standard. Etest endpoints are often difficult to read due to the trailing effect seen with some strains [about 20% of yeasts]. As a result MIC's may tend to be higher than expected so it is important to repeat any “resistant” results in parallel with a control stain or to have them confirmed by another method.
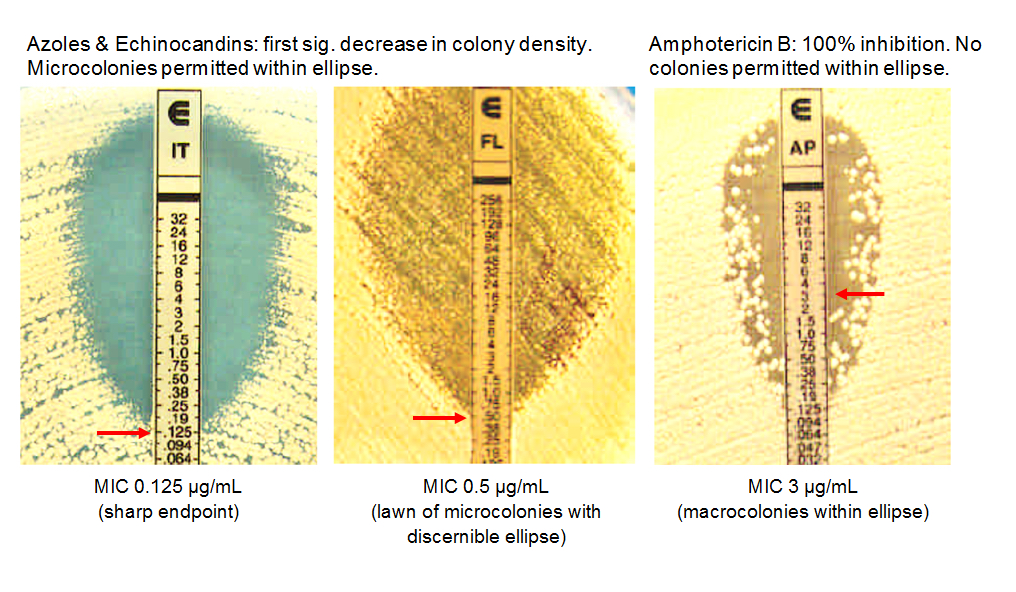
Interpretation of Etests.13Click images below to expand:
Vitek
The Vitek 2 automated system (bioMérieux, France) provides yeast identification and AFST results in 14–18 h. Seven antifungal agents are available for testing, however only fluconazole, caspofungin and voriconazole are approved by the US Food and Drug Administration.11 Studies have reported reproducible and accurate results between the Vitek 2 and CLSI/EUCAST reference methods with essential agreements of 88–98%.11,16-18 However, a limitation of Vitek 2 AST is that the lowest caspofungin concentration (0.25 mg/L) is higher than the Candida glabrata CLSI breakpoint for susceptibility and therefore misclassifies as susceptible C. glabrata isolates with known mechanisms of resistance (i.e., fks hot spot mutations).16
The Micronaut-AM EUCAST AFST (Merlin-Diagnostika, Germany) is a commercially available EUCAST based colorimetric broth microdilution method for six antifungal agents, however there are no published studies comparing its performance with the EUCAST standard. To our knowledge there are no Australasian laboratories using this method and it has not been extensively evaluated.
Tips from the Bench
Inoculum preparation:
For Yeasts (Candida and Cryptococcus)
Sub-culture onto Sabouraud’s Dextrose Agar and incubate for 24-48 hours at 35°C to obtain a freshly grown pure culture.
Use a sterile cotton tip swab to harvest colonies and vortex thoroughly to ensure a homogenous suspension (no clumped cells).For Moulds
Sub-culture to Potato Dextrose Agar slopes and incubate for 7 days at 35°C for most moulds, except Fusarium spp. which should be incubated for 2 days at 35°C then 5 days at 25°C to ensure maximum sporulation (shorter incubation times may be used if results are required urgently bearing in mind the need for sufficient numbers of conidia to harvest).
Use a sterile paster pipette to gently wash the surface of the colony with sterile distilled water or saline (for Aspergillus use 1 drop of Tween 20 as a wetting agent to help disperse the conidia).
For filamentous fungi, which do not sporulate profusely, add one drop of the wetting agent Tween 20 to the sterile distilled water and then break up the mould by vortexing it with small glass beads to make a suitable suspension.
Allow the suspension to stand for a few minutes so that larger hyphal segments have time to settle, then use top homogenous layer to obtain the desired inoculum density.
Inoculating trays
Ensure that yeast cells and conidia Always mix, mix and mix to ensure yeast cells or conidia are evenly distributed through the suspension.
Use a multi-channel pipette.This is important to achieve an even distribution of the inoculum, avoiding skipped wells and for reducing air bubbles.
Incubate trays in moist chamber if not sealed.Reading MICs
Reading antifungal susceptibility results is not an exact science. Artefacts can and do occur, and extensive experience is required to recognise and deal with them. Some common examples are trailing and paradoxical growth.
Skipped wells may occur due to (a) inconsistent inoculum dispensed into wells, (b) poor growth habit of organism, and (c) a manufacturing error when the drug as dispensed into wells. Repeat the test if two or more skipped wells are present.
Some azoles, particularly fluconazole, exhibit a phenomenon known as trailing. Trailing occurs when the turbidity continually decreases as the drug concentration increases but the suspension fails to become optically clear (partial inhibition of growth over an extended range of antifungal concentrations). For most isolates, the difference between reading at 24 hours versus 48 hours is minimal and will not alter the interpretative category (i.e. does not change whether the isolate would be read as “susceptible” or “resistant”). However some isolates show a dramatic rise in MIC over time (e.g. for fluconazole from 0.5 μg/ml at 24 hours to 256 μg/ml at 48 hours). This trailing phenomenon has been reported as occurring in about 5% of isolates,8 however some studies have reported that up to 20% of C. albicans isolates read at 48 hours may show trailing to fluconazole that would alter the interpretation from “susceptible” to “resistant” 6,7. To help resolve this issue the M27-A4 methodology for Candidiasis provided both 24 hour and 48 hour microdilution MIC ranges for the two QC strains and eight systemic antifungal agents. Ideally plates should be read at 24 hours whenever there is sufficient growth. Trailing may also be seen in E-tests as microcolonies growing within the ellipse.
Paradoxical growth may occur in some cases, and is observed as inhibition of fungal growth at a low drug concentration with a resumption of fungal growth at higher antifungal concentrations. This might occur if the drug precipitates out of solution, reducing the available drug concentration. Alternatively the drug might be self-antagonising its receptor. In many cases the true MIC of the isolate can be read by ignoring the growth at higher drug concentrations. However if there is any doubt, the test should be repeated and/or confirmed using a different method.
Summary:
The main practical difficulties with antifungal susceptibility testing are usually with the inoculum preparation and endpoint determination. An inoculum sterility and density check should be done for each test [i.e. spread 10 μL of the inoculum onto a clean SDA plate and count the CFU’s at 24 hours]. This also acts as a growth control for slower growing fungi [i.e. you may have to read some plates at 48 or 72 hours]. If the inoculum is too light or heavy the test should be repeated. Endpoint reading may also be enhanced by the use of colorimetric indicators, plate readers and automated zone readers, which allow for a more quantitative result. No one test is fool proof, if results are unexpected then the test should be repeated for confirmation.
The identity of the culture is often predictive of its in vitro susceptibility, and performing susceptibilities on all isolates that request MC&S is prohibitive in terms of costs and labour requirements. Therefore the decision of which isolates to test should be based on clinical relevance, site (invasiveness) of infection, history of patient antifungal exposure, and the quality of susceptibility data for that species. In many cases the clinical relevance of in vitro antifungal susceptibility results remains difficult to interpret and expert advice from a consulting microbiologist or infectious disease specialist may be required. It is critically important to ensure that valid interpretive criteria have been used (where available). For example, the use of EUCAST breakpoints for Sensititre YeastOne testing may lead to misclassification of isolates as susceptible or resistant, and impede clinical management.
References:
1. CLSI. Reference Method for Broth Dilution Antifungal Susceptibility Testing of Yeasts; Approved Standard-Second Edition. CLSI document M27-A4. CLSI, Pennsylvania, USA 2017.
2. CLSI. Reference Method for Broth Dilution Antifungal Susceptibility Testing of Filamentous Fungi; Approved Standard. CLSI document M38-A3. CLSI, Pennsylvania, USA 2017.
3. CLSI. Performance Standards for Antifungal Susceptibility Testing of Yeasts M60. Wayne, PA, USA: Clinical and Laboratory Standards Institute; 2017
4. CLSI. Epidemiological Cutoff Values for Antifungal Susceptibility Testing, M59, Ed 2. Wayne, PA, USA: Clinical and Laboratory Standards Institute; 2018.
5. Kidd SE, Halliday CL, Morris AJ, et al.,2018. Antifungal susceptibility testing in Australasian clinical laboratories: we must improve our performance. Pathology 50: 257-60.
6. Halliday CL, Chen SC, Kidd SE, et al. 2016. Antifungal susceptibilities of non-Aspergillus filamentous fungi causing invasive infection in Australia: support for current antifungal guideline recommendations. Int J Antimicrob Agents48: 453-8.
7. Talbot JJ, Kidd SE, Martin P, et al. 2015. Azole resistance in canine and feline isolates of Aspergillus fumigatus. Comp Immunol Microbiol Infect. 42: 37-41.
8. Patel R, Mendrick C, Knapp CC, et al. 2007. Clinical Evaluation of the Sensititre YeastOne Plate for Testing Susceptibility of Filamentous Fungi to Posaconazole.JClin Microbiol.45: 2000-1.
9. Morace G, Drago M, Scaltrito MM, et al. 2007. In Vitro Activity (MIC and MFC) of Voriconazole, Amphotericin B, and Itraconazole Against 192 Filamentous Fungi: The GISIA-2 Study. J.Chemother.19: 508-13,
10. Cuenca-Estrella M, Gomez-Lopez A, Alastruey-Izquierdo A, et al. 2010. Comparison of the Vitek 2 antifungal susceptibility system with the clinical and laboratory standards institute (CLSI) and European Committee on Antimicrobial Susceptibility Testing (EUCAST) Broth Microdilution Reference Methods and with the Sensititre YeastOne and Etest techniques for in vitro detection of antifungal resistance in yeast isolates. J Clin Microbiol. 48:1782-6.
11. Albataineh MT, Sutton DA, Fothergill AW, Wiederhold NP. 2016. Update from the Laboratory: Clinical Identification and Susceptibility Testing of Fungi and Trends in Antifungal Resistance. Infect Dis Clin North Am. 30: 13-35.
12. Espinel-Ingroff A, Pfaller M, Messer SA. et al. 1999. Multicenter comparison of the Sensititre YeastOne colorimetric antifungal panel with the National Committee for Clinical Laboratory Standards M27-A reference method for testing clinical isolates of common and emerging Candida spp., Cryptococcus spp., and other yeasts and yeast-like organisms. J Clin Microbiol.37: 591-5.
13. Etest Technical Guide 4b AB Biodisk, Sweden.
14. Chen CA, O’Donnell ML, Gordon S, Gilbert GL. 1996. Antifungal susceptibility testing using Etest: comparison with broth macrodilution technique. J Antimicrob Chemo.37: 265-73.
15. Arikan S, Gur D, Akova M. 1997. Comparison of Etest, microdilution and colorimetric dilution with reference broth macrodilution method for antifungal susceptibility testing of clinically significant Candida species isolated from immunocompromised patients. Mycoses 40: 291-6.
16. Astvad KM, Perlin DS, Johansen HK, Jensen RH, Arendrup MC. 2013. Evaluation of caspofungin susceptibility testing by the new Vitek 2 AST-YS06 yeast card using a unique collection of FKS wild-type and hot spot mutant isolates, including the five most common Candida species. Antimicrob Agents Chemother, 57: 177-82.
17. Pfaller MA, Diekema DJ, Procop GW, Rinaldi MG. 2013. Comparison of the Vitek 2 yeast susceptibility system with CLSI microdilution for antifungal susceptibility testing of fluconazole and voriconazole against Candida spp., using new clinical breakpoints and epidemiological cutoff values. Diagn Microbiol Infect Dis, 77:37-40.
18. Peterson JF, Pfaller MA, Diekema DJ, et al,. 2011. Multicenter comparison of the Vitek 2 antifungal susceptibility test with the CLSI broth microdilution reference method for testing caspofungin, micafungin, and posaconazole against Candida spp. J Clin Microbiol, 49: 1765-71 -
Mycology specimen collection video
This 14 minute video describes specimen collection techniques from skin, hair and nails for the laboratory diagnosis of tinea, ringworm and onychomycosis.
This 14 minute video describes specimen collection techniques from skin, hair and nails for the laboratory diagnosis of tinea, ringworm and onychomycosis.
-
Specimen collection and processing
-
Culture techniques and media
ASM Guidelines for Assuring Quality of Medical Mycology culture media
- Bird seed agar
- Bromocresol purple milk solids agar
- Creatinine dextrose bromothymol blue thymine (CDBT) media
- Canavanine glucose bromothymol blue (CGB) media
- Cornmeal agar
- Cornmeal glucose sucrose agar
- Czapek Dox agar
- Modified Dixon’s agar
- Hair perforation test
- Lactritmel agar
- Littman oxgall agar
- Malt extract agar
- 1% Peptone agar
- Potato dextrose agar
- Rice grain slopes
- Sabouraud’s dextrose agar (SDA) + cycloheximide and antibiotics
- Sabouraud’s dextrose agar (SDA) + antibiotics
- Sabouraud’s dextrose agar (SDA) 5% salt
- Tap water agar
- Urea agar with 0.5% glucose
- Vitamin free agar
-
Microscopy techniques and stains