Zygomycosis
Clinical Manifestations:
Zygomycosis in the debilitated patient is the most acute and fulminate fungal infection known. The disease typically involves the rhino-facial-cranial area, lungs, gastrointestinal tract, skin, or less commonly other organ systems. It is often associated with acidotic diabetes, starvation, severe burns, intravenous drug abuse, and other diseases such as leukemia and lymphoma, immunosuppressive therapy, or the use of cytotoxins and corticosteroids, therapy with desferrioxamine (an iron chelating agent for the treatment of iron overload) and other major trauma. The infecting fungi have a predilection for invading vessels of the arterial system, causing embolization and subsequent necrosis of surrounding tissue. A rapid diagnosis is extremely important if management and therapy are to be successful.

Rhinocerebral zygomycosis showing involvement of the palate.
1. Rhinocerebral zygomycosis:
Predisposing factors include uncontrolled diabetes mellitus or acidosis, steroid induced hyperglycemia, especially in patients with leukemia and lymphoma, renal transplant and concomitant treatment with corticosteroids and azathioprine. Infections usually begin in the paranasal sinuses following the inhalation of sporangiospores and may involve the orbit, palate, face, nose or brain.
2. Pulmonary zygomycosis:
Predisposing conditions include haematological malignancies, lymphoma and leukemia, or severe neutropenia, treatment with cytotoxins and corticosteroids, desferrioxamine therapy; diabetes and organ transplantation. Infections result by inhalation of sporangiospores into the bronchioles and alveoli, leading to pulmonary infraction and necrosis with cavitation.
3. Gastrointestinal zygomycosis:
A rare entity, usually associated with severe malnutrition, particularly in children, and gastrointestinal diseases which disrupt the integrity of the mucosa. Primary infections probable result following the ingestion of fungal elements and usually present as necrotic ulcers.
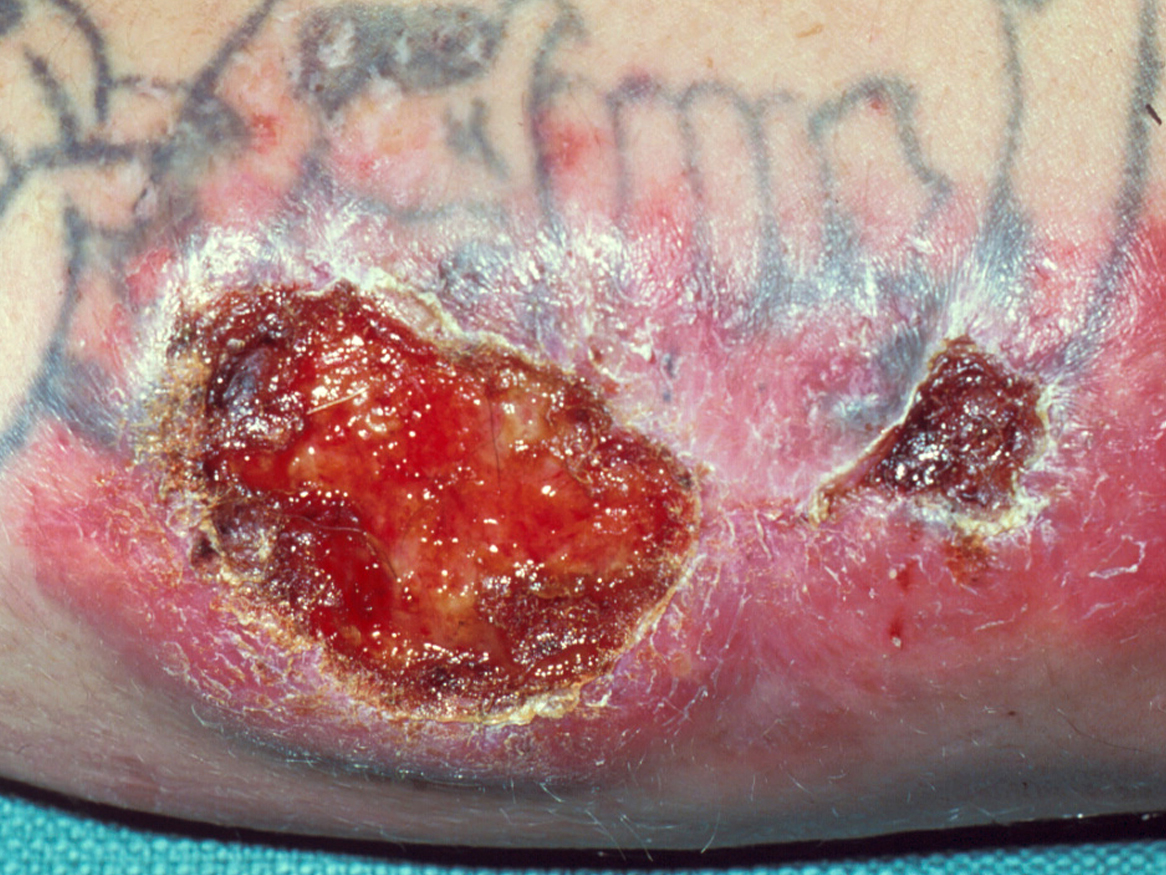
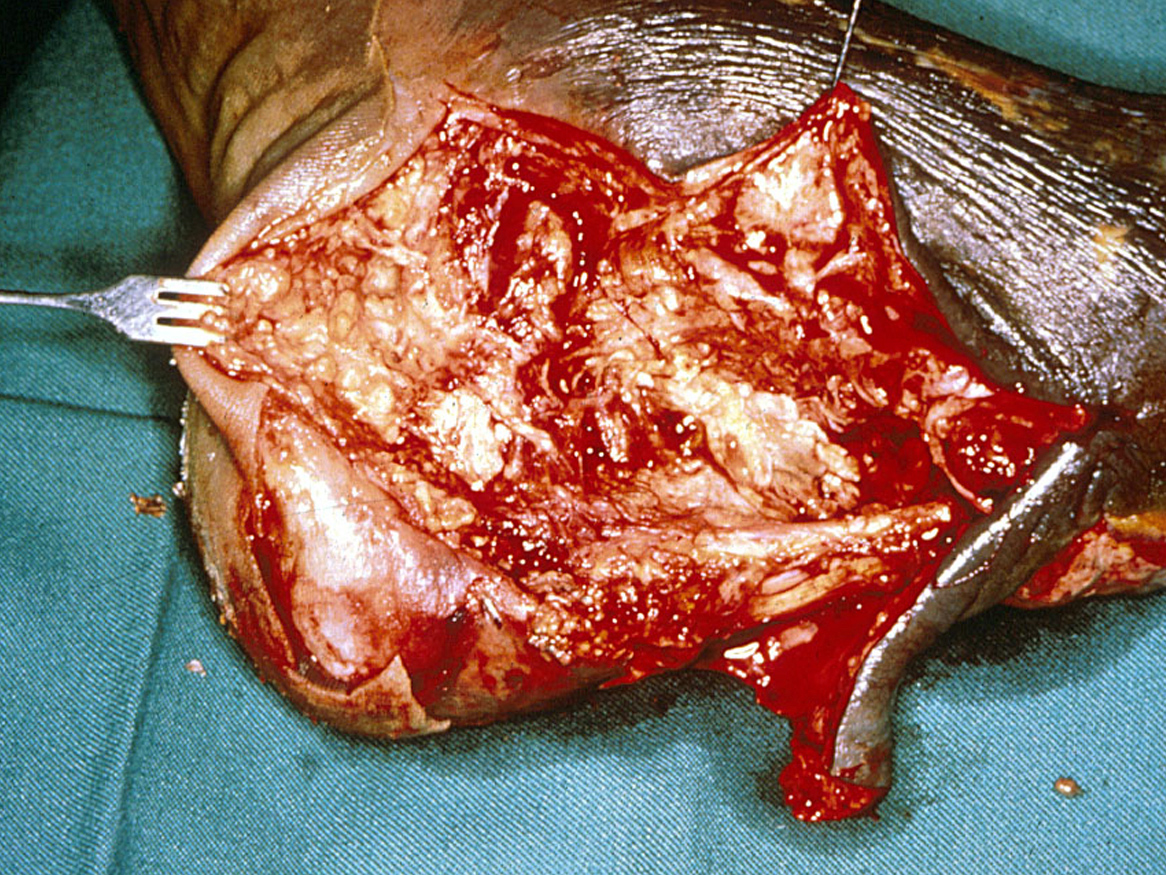
4. Cutaneous zygomycosis:
Local traumatic implantation of fungal elements through the skin, especially in patients with extensive burns, diabetes or steroid induced hyperglycemia and trauma. Lesions vary considerably in morphology but include plaques, pustules, ulcerations, deep abscesses and ragged necrotic patches.
Click images below to expand:

5. Disseminated zygomycosis:
May originate from any of the above, especially in severely debilitated patients with haematological malignancies, burns, diabetes or uraemia.
6. Central Nervous System alone:
Intravenous drug abuse. Traumatic implantation leading to brain abscess.
Laboratory Diagnosis:
1. Clinical Material:
Skin scrapings from cutaneous lesions; sputum and needle biopsies from pulmonary lesions; nasal discharges, scrapings and aspirates from sinuses in patients with rhinocerebral lesions; and biopsy tissue from patients with gastrointestinal and/or disseminated disease.
Warning: zygomycetous fungi have primitive coenocytic hyphae that will often be damaged and become non-viable during the biopsy procedure (especially scrapings and aspirates), or by the chopping up or tissue grinding process in the laboratory. This is why zygomycetous fungi that are clearly visible in direct microscopic or histopathological mounts are often difficult to grow in culture from clinical specimens. If on clinical and/or radiological evidence zygomycosis is suspected then try to avoid excessive tissue damage when collecting the specimen and in the laboratory gently tease the tissue apart and inoculate it directly onto the isolation media. If you are not sure hold the specimen in saline or BHI broth until the results of the direct microscopy or frozen histology sections are known. If zygomycetous hyphae are present proceed as above, otherwise homogenised the specimen and plate out.
Click images below to expand:
3. Culture:
Inoculate specimens onto primary isolation media, like Sabouraud's dextrose agar. Most zygomycetes are sensitive to cycloheximide (actidione) and this agent should not be used in culture media. Look for fast growing, white to grey or brownish, downy colonies.
Interpretation:
Despite being recognised as common laboratory contaminants, zygomycetes are infrequently isolated in the clinical laboratory. Therefore, in patients with any of the above predisposing conditions, especially diabetes or immunosuppression and/or clinical symptoms, the isolation of any zygomycete fungus should be regarded as potentially significant. Obviously, in patients without predisposing conditions, the isolation of a zygomycete from a non-sterile site, such as skin or sputum, must be interpreted with caution, especially in the absence of direct microscopy.
4. Serology:
There are currently no commercially available serological procedures for the diagnosis of zygomycosis. Although some laboratories have developed ELISA tests for the detection of antibodies to Zygomycetes.
5. Identification:
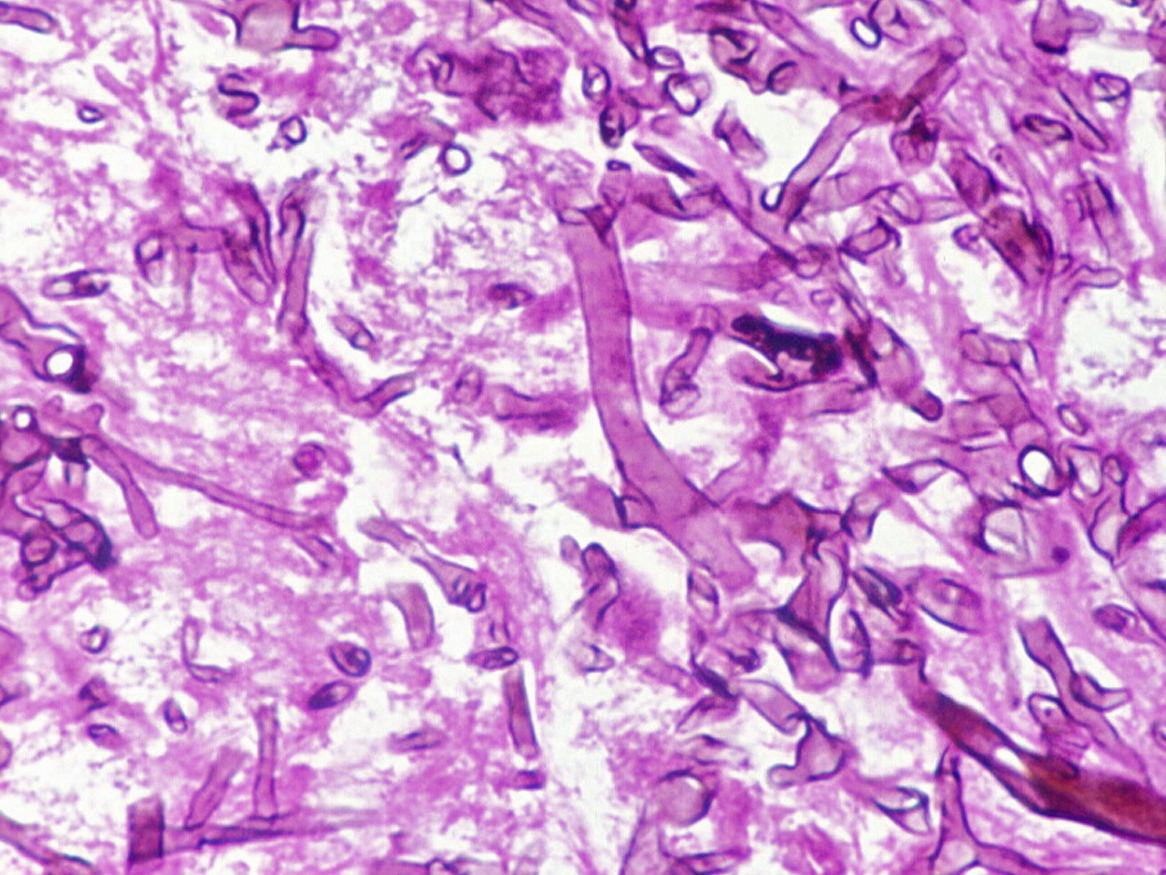
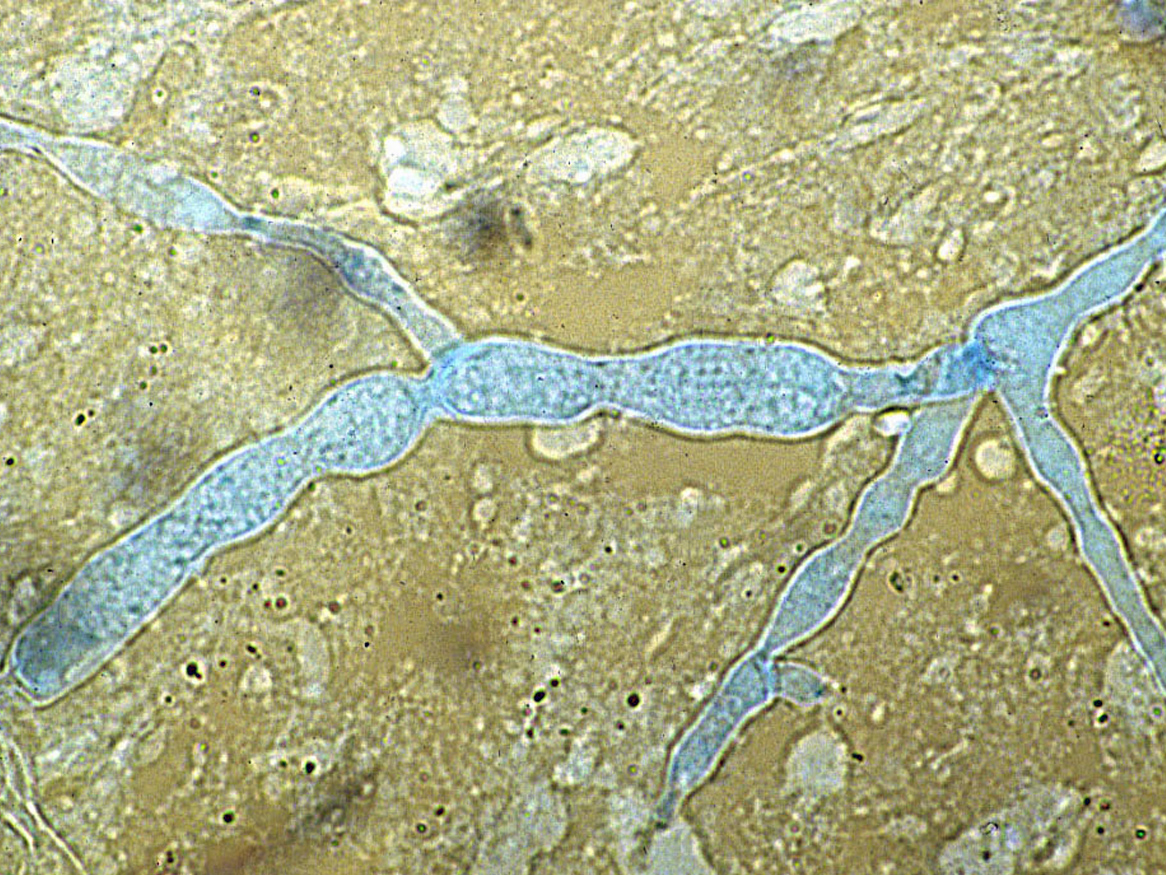
Zygomycetes are usually fast growing fungi characterised by primitive coenocytic (mostly aseptate) hyphae. Asexual spores include chlamydoconidia, conidia and sporangiospores contained in sporangia borne on simple or branched sporangiophores. Sexual reproduction is isogamous producing a thick-walled sexual resting spore called a zygospore.
Most isolates are heterothallic i.e. zygospores are absent, therefore identification is based primarily on sporangial morphology. This includes the arrangement and number of sporangiospores, shape, colour, presence or absence of columellae and apophyses, as well as the arrangement of the sporangiophores and the presence or absence of rhizoids. Growth temperature studies (25,37,45C) can also be helpful. Tease mounts are best, use a drop of 95% alcohol as a wetting agent to reduce air bubbles. Laboratory identification of some zygomycetous fungi, especially Apophysomyces elegans and Saksenaea vasiformis may be difficult or delayed because of the mould's failure to sporulate on the primary isolation media or on subsequent subculture onto potato dextrose agar. Sporulation may be stimulated by the use of nutrient deficient media, like cornmeal-glucose-sucrose-yeast extract agar, Czapek Dox agar, or by using the agar block method on water agar.
6. Causative agents:
Lichtheimia corymbifera, Apophysomyces elegans, Cunninghamella bertholletiae, Mortierella wolfii, Mucor sp.,Rhizomucor pusillus, Rhizopus arrhizus, Rhizopus sp., Saksenaea vasiformis.
Further reading:
Ellis, DH. 2005. Systemic Zygomycetes – Mucormycosis. Chapter 33. In Topley and Wilson’s Microbiology and Microbial Infections: Medical Mycology, 10th edition, Hodder Arnold London. pp 659-686.
Kwon-Chung KJ and JE Bennett 1992. Medical Mycology Lea & Febiger.
Rippon JW. 1988. Medical Mycology WB Saunders Co.
Back to Subcutaneous Mycoses Back to Opportunistic Systemic Mycoses